“Know how to solve every problem that has been solved.”“What I cannot create, I do not understand.”— Richard Feynman
Project: Gamma Knife Dose Simulation
Projects
Two hundred weak beams, one hot point: the geometry of stereotactic radiosurgery, computed and validated. Stack: Python · NumPy · Monte Carlo attenuation check. A physics teaching model — not a treatment-planning tool.
What this is
A Gamma Knife treats a brain lesion without a scalpel by pointing roughly two hundred
cobalt-60 beams at one point. Each beam on its own is too weak to destroy tissue —
it deposits a long, gentle stripe of dose on its way through the head. But every beam
passes through the same few cubic millimeters, and there the doses add. One beam burns
a line; two hundred burn a point. This project builds the dose model from three pieces
of freshman physics — exponential attenuation, inverse-square spreading, a collimated
beam profile — and then quantifies exactly how the point wins over the lines. Lars
Leksell proposed the idea in 1951 and treated the first patients with a prototype in
the 1960s; the collimator sizes here (4, 8, 16 mm) are the real ones.
The model, and its edges
Each beam is a narrow cone of 1.25 MeV photons (the average of cobalt-60's
1.17 and 1.33 MeV lines) converging on the isocenter from a source
40 cm away. At a point p inside a spherical
water phantom of radius 8 cm, the primary dose from one beam is
Di(p)=e−μdi(p)(ri(p)SAD)2exp(−2σ2bi(p)2),
where di is the tissue path length from skull entry,
ri the distance from the source, bi the distance off the
beam's central axis, and σ is set by the collimator width
(FWHM = 4, 8, or 16 mm). The attenuation coefficient is the NIST value for
water at 1.25 MeV, μ/ρ=0.0632cm2/g. The total
dose is the sum over beams whose axes are spread over a helmet-like spherical cap.
Stated plainly, this is a primary-photon model: it tracks the photons that arrive
unscattered and ignores what happens after they interact. A full Monte Carlo
transport calculation adds Compton-scattered dose, electron buildup at the surface,
and bone/air heterogeneities — corrections a clinic cannot ignore and this page can,
because the phenomenon being studied (dose concentration by convergence) lives
entirely in the geometry.
MU = 0.0632 # 1/cm, water at 1.25 MeV (NIST mass attenuation x 1 g/cm^3)R_HEAD = 8.0 # cm, spherical water phantomSAD = 40.0 # cm, source-to-isocenter distancedef beam_dose(points, u, sigma): """Primary dose of one beam (axis through origin, direction u, source at SAD*u) at an array of points, shape (M, 3).""" s = SAD * u w = points - s # source -> point r = np.linalg.norm(w, axis=1) v = w / r[:, None] # ray-sphere entry: |s + t v| = R_HEAD, smaller positive root b_ = np.einsum("j,ij->i", s, v) disc = b_**2 - (SAD**2 - R_HEAD**2) t_entry = -b_ - np.sqrt(np.maximum(disc, 0.0)) depth = np.maximum(0.0, r - t_entry) # path length in tissue # off-axis distance from the central axis (line through origin along u) proj = np.einsum("ij,j->i", points, u) b_axis = np.linalg.norm(points - proj[:, None] * u, axis=1) return np.exp(-MU * depth) * (SAD / r)**2 * np.exp(-b_axis**2 / (2 * sigma**2))
Validation before physics
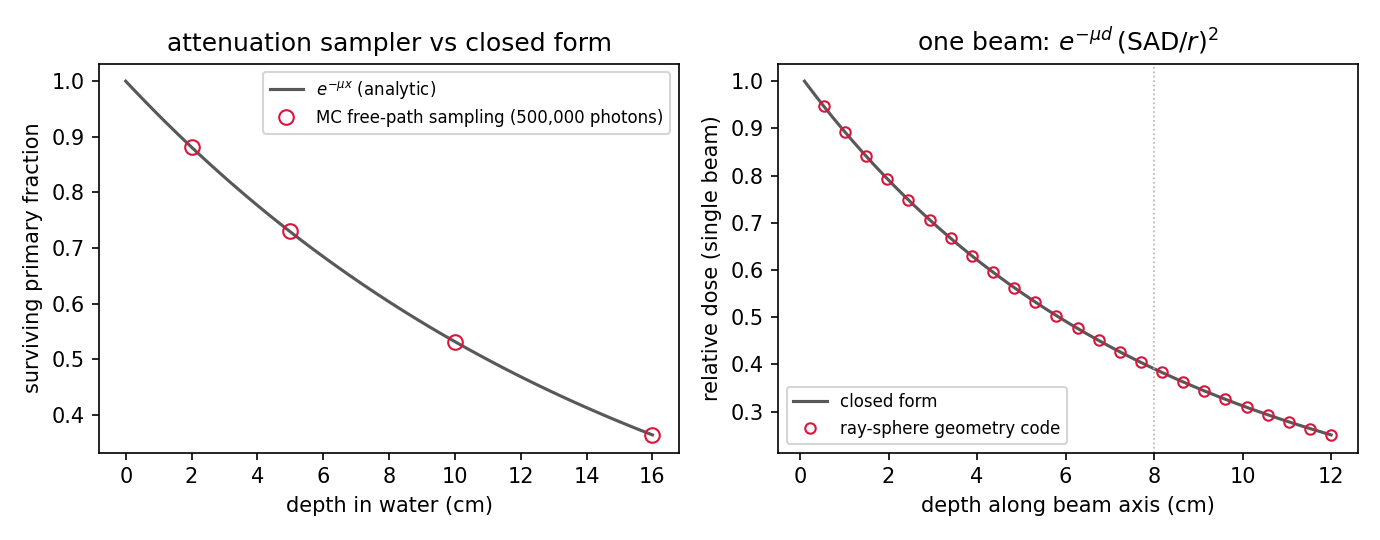
Two checks, both against closed forms. The vectorized ray-sphere geometry is compared
with the hand-derived on-axis formula e−μ(R−z)(SAD/(SAD−z))2
— agreement to 4×10−16, machine precision. And a small Monte Carlo
samples 500,000 photon free paths from ℓ=−lnξ/μ and counts
survivors past each depth; the survival fractions land on e−μx to 0.17%,
which is the expected statistical noise. The attenuation model and its implementation
are both doing what they claim.
[1] geometry vs closed form max |err| = 4.44e-16[2] MC survival vs exp(-mu x), 500,000 photons: x = 2.0 cm MC 0.88206 analytic 0.88126 x = 5.0 cm MC 0.73033 analytic 0.72906 x = 10.0 cm MC 0.53163 analytic 0.53153 x = 16.0 cm MC 0.36395 analytic 0.36378 max relative deviation = 0.17%
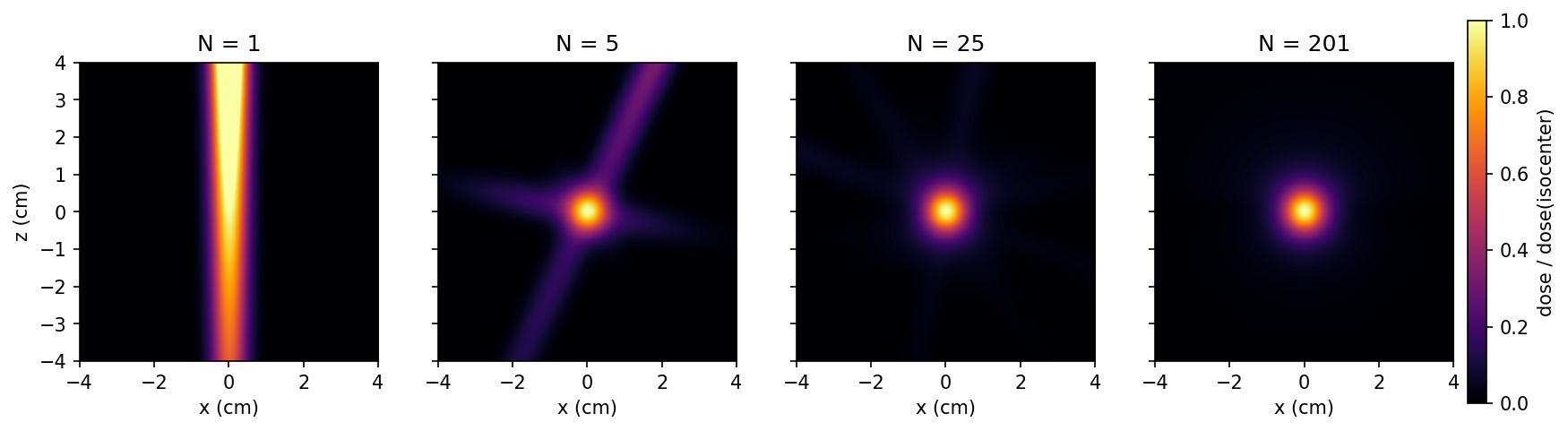
The picture that is the whole idea
The same slice through the isocenter, computed with 1, 5, 25, and 201 beams, each map
normalized to its own isocenter dose. With one beam the "treatment" is a corridor of
full-strength dose straight through the head. Five beams make a star whose arms carry
a fifth of the dose each. By 201, the arms have faded below 2% and what remains is a
ball of dose the size of the collimator setting.
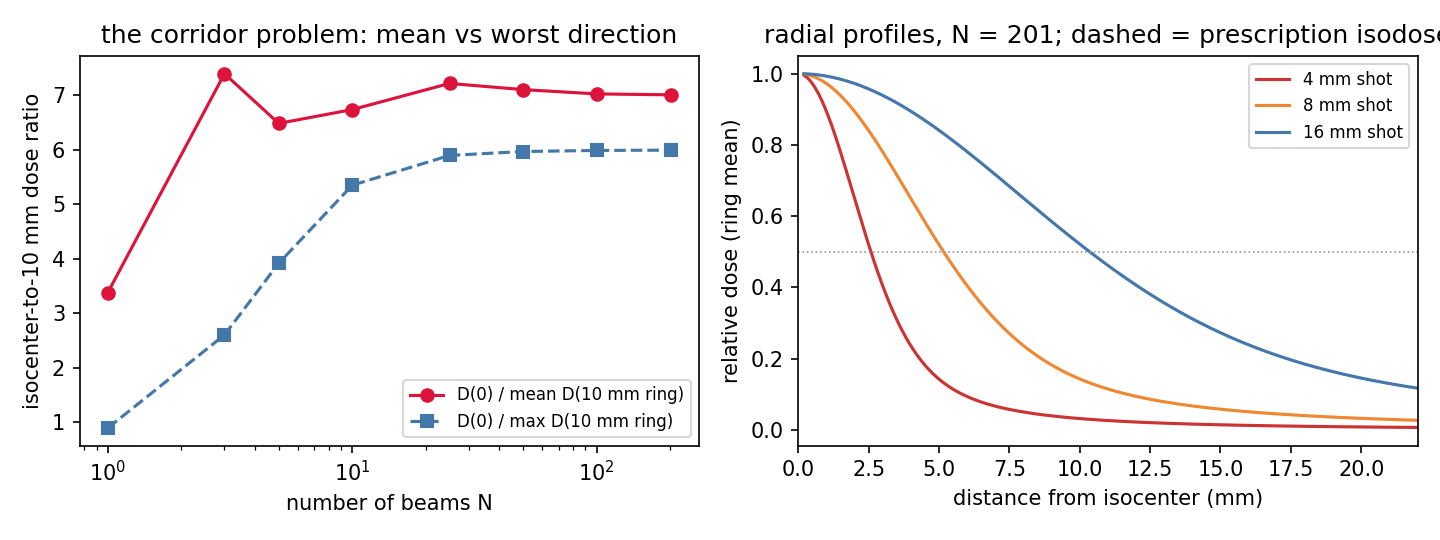
The numbers underneath sharpen the story, and the first row contains the best fact on
this page: with a single beam, the isocenter-to-worst-point ratio at 10 mm is
0.89 — less than one. The target is not even the hottest place on
that ring. Upstream tissue sits closer to the source and behind less attenuating
material, so a single beam always deposits more dose on the way in than at the lesion.
Convergence doesn't just spare healthy tissue; it is the only way to make the target
the maximum of the dose field at all.
[3] falloff vs number of beams (8 mm collimator): N D0/mean(5mm) D0/mean(10mm) D0/max(10mm) 1 1.60 3.38 0.89 <- target is NOT the hottest point 3 2.02 7.40 2.60 5 1.90 6.48 3.92 10 1.89 6.74 5.35 25 1.94 7.22 5.90 201 1.92 7.01 5.99 <- worst direction 6x colder[4] 50% isodose radius (N = 201) per collimator: 4 mm shot: r50 = 2.57 mm penumbra 80->20% = 2.87 mm 8 mm shot: r50 = 5.18 mm penumbra 80->20% = 5.86 mm 16 mm shot: r50 = 10.29 mm penumbra 80->20% = 11.71 mm[5] Co-60 after 5 years: 0.5181 of initial activity (3.5 Gy/min fresh -> 1.81 Gy/min; treatment times x1.93)
Note what the left panel says about diminishing returns: the mean falloff is
already saturated by a handful of beams, but the worst-direction falloff — the
number that decides whether some corridor of healthy tissue takes real dose — keeps
improving until about 25 beams and only then plateaus near 6×. The extra 176 beams buy
insurance in every direction at once, plus the freedom to block individual beams that
would pass through something delicate.
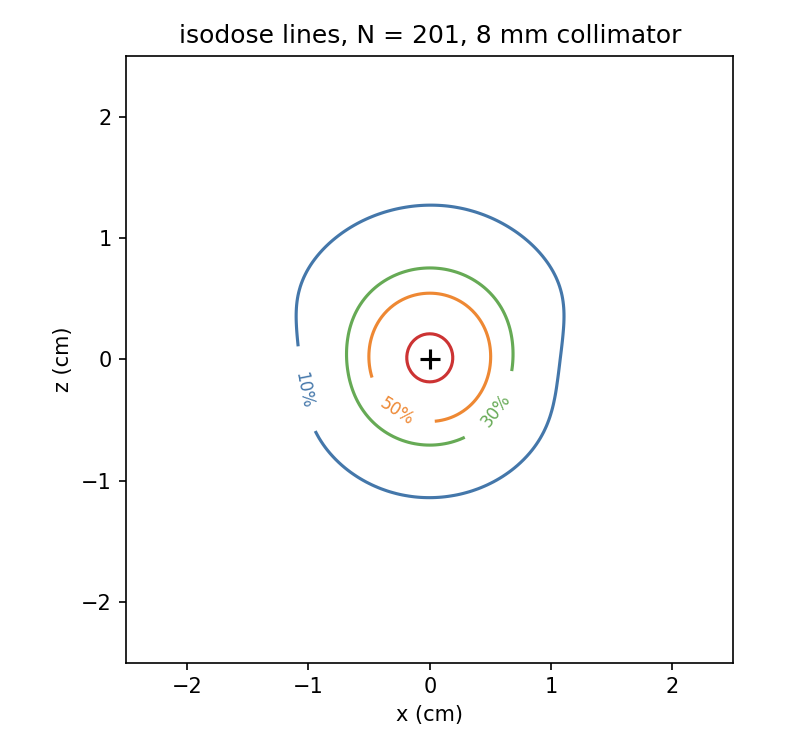
Reading it like a treatment plan
Clinical Gamma Knife plans are traditionally prescribed to the 50% isodose
line — the surgeon draws the lesion, and the plan arranges for that surface to
receive half the maximum dose. In this model the 50% radius comes out at 2.6, 5.2, and
10.3 mm for the 4, 8, and 16 mm collimators — the shot size tracks the
collimator, as it should. The penumbra, the shell where dose falls from 80% to
20%, is 3 to 12 mm wide: that is the physics-imposed price of a Gaussian beam
profile, and the reason radiosurgery targets are contoured in millimeters. The
contours are slightly taller than they are wide — a real effect of the helmet
geometry, since beams arrive from the upper hemisphere only and thin the dose along
the polar axis less than the equatorial one.
One more piece of working arithmetic: cobalt-60 has a 5.27-year half-life, so after
five years the sources hold 2−5/5.27=0.518 of their activity and every
treatment takes 1.93× as long. That is the actual economics of these machines — the
sources are swapped roughly every five to seven years not because they stop working
but because treatment time doubles.
Try First
Each prompt asks a checkable question about the working code or math
above — predict an output, derive a sign, state an invariant, find a
bug. Commit to an answer before clicking "reveal." That commitment is
the whole point: if your answer matched, you understand the piece you
were looking at; if it didn't, that's the part worth re-reading.
predict
Before looking at the falloff table: with a single beam and the target at
the center of the head, where is the maximum of the dose field?
answer
On the beam axis, upstream of the target, just inside the skull — where tissue is
closest to the source and shielded by the least material. Both factors,
e−μd and 1/r2, decrease monotonically with depth,
so a single beam's dose maximum is always at the entry surface. The table's
D0/Dmax=0.89 at 10 mm is that fact leaking into the ring
metric.
why does this work
Each individual beam's depth profile is the same gentle exponential no matter how
many beams there are. Why does adding beams sharpen the falloff around the target?
hint
Normalize by the isocenter dose and ask what happens at an off-target point.
answer
Every beam contributes its full profile value at the isocenter, so the center
collects N full shares. An off-target point sits in the Gaussian tail
of almost every beam — only the one or two beams whose axis happens to pass nearby
contribute more than a sliver. So the center grows like N while a
generic off-target point grows like N times a small tail value, and
the corridors of individual beams get diluted by the normalization. The
exponential never changed; the bookkeeping did.
what if
The lesion sits 1 cm under the skull instead of at the center. What breaks in
the symmetric-helmet plan, and what would you change?
answer
Beams entering on the near side reach the target through almost no tissue while
far-side beams cross ~14 cm and arrive attenuated by
e−0.0632⋅14≈0.41 — so the dose ball becomes lopsided
and the hot spot shifts toward the near surface, uncomfortably close to the skull
and scalp. Real plans reweight or block beams (and modern machines move the
patient between multiple isocenters) precisely to rebalance this. Implementing the
reweighting is the optimization extension below.
Extensions
The model is deliberately minimal; every one of its omissions is a project.
Compton scatter by Monte Carlo. The free-path sampler is already
validated; add Klein–Nishina sampling of the scattering angle and energy, transport
the scattered photon, and measure how much dose the primary-only model misplaces —
the classic buildup region near the surface should appear on its own.
Beam-weight optimization. For an off-center target, choose per-beam
weights minimizing dose at specified organ-at-risk points subject to full dose at the
target — a small constrained least-squares problem, solvable with
gradient descent or as a quadratic program.
Shot packing. Real lesions are not spheres. Cover an irregular 3D
target with multiple isocenters of different collimator sizes and score the plan with
the clinical conformity indices (RTOG, Paddick).
A skull, not a water ball. Add a 6 mm bone shell
(μ about 1.9× water's at this energy) and an air-filled sinus, and
watch the isodose lines dent.
The proton comparison. Photons attenuate exponentially; protons stop
at a depth and deposit most of their energy in the last few millimeters (the Bragg
peak). Build the same figures for a scanned proton beam and compare the two ways
physics offers to concentrate dose.
Everything above is generated by scripts/projects/gamma_knife.py — the
figures, the falloff table, and the validation numbers come from one run of the model,
not from a textbook screenshot.